Did your provider recently mention an external cephalic version (ECV) to you because your baby is breech? Or maybe you heard someone online talking about ways to turn a breech baby? You’re in the right place. An ECV is exactly what they’re talking about. And if your baby is breech, either right now or closer to delivery, you’ll want to know about ECVs so you can decide if it’s something you’d like to try. If your provider doesn’t bring it up? You bring it up! I’d encourage you to ask them about ECV and have the conversation.
Who is The Labor Mama and Why Am I Here?
Hey friend! I’m Lo – also known around here and social media as The Labor Mama. I’ve spent my nursing career in labor, delivery, and postpartum, have birthed 4 of my own babies, have labored thousands of mamas at the bedside, have taught hundreds of students online, and have even delivered a few speedy little babies with my bare hands (oops).
Here at TLM, I offer online classes to empower you the way everyone should be. The education + support I offer gives you experience, evidence, and empathy; you’re getting all of my years of “clinical” RN knowledge, beautifully combined with my real experiences as a mama and a nurse. These are not your average hospital classes (those won’t do it, I promise), and honestly, birth, postpartum, and breastfeeding don’t follow a textbook or protocol anyway. You need to know so much more than that!
If you want to connect with me further, head to Instagram. There are hundreds of thousands of us over there learning together daily.
A note: This post may include affiliate links. This means if you make a purchase after clicking a link, I will earn a small commission (thank you)! Rest assured, this comes at no additional cost to you. You can read TLM’s full disclosure here.
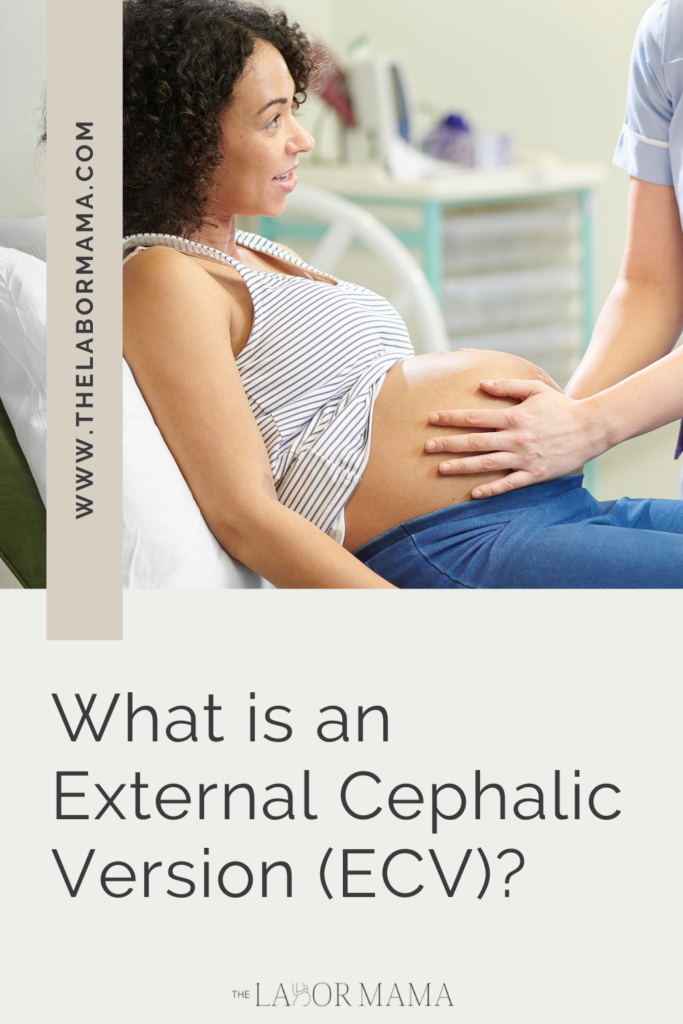
What is external cephalic version?
An external cephalic version is a procedure in which your provider uses their hands on the outside of your belly to try and manually turn your baby from breech to vertex position. Breech = butt or feet down, while vertex = head down. Though vaginal breech birth can be done, it is rare in the US and it comes with elevated risks of cord prolapse and fetal injury during delivery. It can also be hard to find a provider to assist you in one. However, if an ECV is successful (meaning baby flips to head down), this greatly increases your chance of successful vaginal birth.

Success rate of ECVs
It is hard to say exactly how successful an ECV may be. In first time birthing people, the ECV success rate hovers around 33%. However, the success rate is closer to 60% in people who have had a prior birth. Overall, success rates have also been shown to improve if the care provider uses a tocolytic before the procedure. A tocolytic is a drug that can stop uterine contractions. Using a drug like this (commonly administered via an IV) ensures that the uterus is fully relaxed before trying to turn the baby.
Should you have an ECV?
The American College of Obstetricians and Gynecologists (ACOG) supports ECV, particularly as a way to continue to bring down the elevated cesarean rate in the US. But, they do recommend that each of these decisions be made on a case-by-case basis.
Are you a good candidate?
When an ECV is done, it is usually performed around 37-weeks (full term). Research shows that this is the best time to attempt an ECV. They are not usually done before this point, because some babies will continue to turn on their own. The belief is that at 37 weeks there is still enough room to move the baby, but that there isn’t so much room that the baby will easily return to the breech position on their own.
Typically, you may be a candidate for an ECV if you have a:
- baby that is 37 weeks along
- singleton pregnancy (meaning one baby)
- normal amount of amniotic fluid
- baby has no birth defects and a reassuring heart rate
- pelvis with no known abnormalities
- baby whose head is in a flexed position.
It’s also important to note that a prior cesarean birth does not mean you cannot have an ECV either!
Here are some reasons you may not be able to have or consider an ECV:
- Your amniotic fluid levels are too low
- Your waters have broken
- You have experienced recent vaginal bleeding
- You have a placenta previa condition
- You are pregnant with more than 1 baby
- Your baby’s heart rate is irregular
- Your uterus is abnormally shaped or has a septum
- It’s already been established that you need to deliver via cesarean
How does the ecv procedure go?
If you are able to attempt an ECV, it will be done at the hospital, near an operating room. A rare risk (about 1 in 200) of the ECV is the need for immediate cesarean birth if your baby’s heart rate becomes non-reassuring during the process. So when you attempt an ECV you will be admitted, given an IV, consented for a c-section, and possibly prepped a little bit.
Before the ECV can begin, your care team will want to monitor the baby. This will be done via external monitors, usually for about 25-40 minutes. One monitor will be placed on your belly to continuously monitor baby’s heart rate. Another monitor will be placed near the top of your uterus (the fundus) to assess the presence of any contractions.

Most commonly, I have seen the procedure performed with two providers. You may be administered a tocolytic to stop any contractions you may be having. You may also be offered IV pain medication. The baby’s heart rate will be monitored throughout the procedure and ultrasound will likely be used too. When everyone is ready, your providers will place their hands on the outside of your stomach and then attempt to turn the baby. This may take a few minutes (maybe 10 or so) as they try moving in a few different directions.
Is ECV done with an epidural?
ACOG recently updated their guidelines to recommend that you be allowed to consider an epidural or spinal during the ECV procedure. Evidence shows that this may increase the ECV success rate. If you are interested in this for your ECV, please, ask about this possibility as well.
How long is the ECV procedure?
An ECV, even when successful, can take 2+ hours. This is because you are admitted and monitored before the ECV and baby is also monitored after the ECV. If you use an epidural or spinal for your ECV, you can expect the whole procedure to be even longer.
Is ECV painful?
Many will tell you that an ECV, successful or not, is very uncomfortable and/or painful. The pressure from the provider(s) can be painful and it can cause uterine cramping. Even if your ECV is done with pain medication or epidural anesthesia, you may still find that you are sore in the days after.
What if the ECV doesn’t work?
The majority of providers will recommend a cesarean birth for a baby that remains breech at term. If you find yourself in this place, I’d encourage you to do some research about gentle cesareans. They can be a really beautiful way to take ownership and control over your cesarean birth experience.
Do you want a birth plan template that includes all the different components of a gentle cesarean? You can snag one here.
The takeaway on external cephalic version
Whether or not to attempt an external cephalic version is such a personal decision. It will likely depend on so many things, including your personal feelings about vaginal birth vs. cesarean birth, your provider’s confidence in the process, and your assessment of your level of risk. Talk to your provider. Consider your priorities, your hopes, what the research says. There isn’t a wrong choice here, but I do hope that your choice is informed.
More resources (and freebies!) for you to take a peek at:
- Comprehensive Birth Plan and Birth Priorities templates
- A complete Third Trimester Checklist
- The RN + mama of 4 Ultimate Packing List
- The Labor Mama online birth, baby and breastfeeding classes for every family