If you’re into the end of your third trimester, it’s pretty likely you are starting to feel some contractions. And when you do, you’re probably asking what we all ask: “Is this labor” or “what type of contraction is this?” I remember those days. Even as a labor nurse who knows all the things, it’s so different to actually be the body experiencing what you teach about! And it IS hard to understand the difference between the types of contractions and what they all mean.
Let’s get into all of it for you. When we’re done, you’re going to know what the different contraction types are, what they may feel like or how they “present” (that’s our clinical term), and what they might mean for you in that moment (or in the moments to come).
This article covers:
- What is a contraction?
- What are the different types of labor contractions?
- What are Braxton Hick’s contractions?
- What is Prodromal Labor?
- What are false labor contractions?
- What are true labor contractions?
- How do you time contractions?
- When should you go to the hospital?
Who is The Labor Mama and Why Am I Here?
Hey friend! I’m Lo – also known around here and social media as The Labor Mama. I’ve spent my nursing career in labor, delivery, and postpartum, have birthed 4 of my own babies, have labored thousands of mamas at the bedside, have taught hundreds of students online, and have even delivered a few speedy little babies with my bare hands (oops).
Here at TLM, I offer online classes to empower you the way everyone should be. The education + support I offer gives you experience, evidence, and empathy; you’re getting all of my years of “clinical” RN knowledge, beautifully combined with my real experiences as a mama and a nurse. These are not your average hospital classes (those won’t do it, I promise), and honestly, birth, postpartum, and breastfeeding don’t follow a textbook or protocol anyway. You need to know so much more than that!
If you want to connect with me further, head to Instagram. There are hundreds of thousands of us over there learning together daily.
A note: This post may include affiliate links. This means if you make a purchase after clicking a link, I will earn a small commission (thank you)! Rest assured, this comes at no additional cost to you. You can read TLM’s full disclosure here.
What is a contraction?
Let’s start with some basics. The uterus is a muscle, right? Basic biology tells us that muscles have the ability to contract, which you know that muscles all over your body do all of the time. Your uterus is no different! It’s been contracting on and off throughout your menstrual cycles for years – that’s your period cramps. And now that you’re pregnant, that uterine muscle is doing the same thing.
What hormones cause contractions?
There are two main things that can act on the uterus to cause contractions – prostaglandins and oxytocin. Your body makes both of them, and when present at the right time and in the right amounts, they can cause labor to start (or strengthen). When contractions aren’t happening, or if you need more contractions or stronger contractions, your care team can actually give you medicines that can help. This is known as:
- Induction: Causing labor to start when nothing is yet going on/no contractions are present and labor has not begun
- Augmentation: Trying to increase the strength or frequency of contractions once labor has already begun
What medications cause contractions?
For induction and augmentation situations, there are prostaglandin medications and there is synthetic oxytocin (Pitocin or Syntocinon). Either of these could be suggested or used to cause contractions. Membrane stripping (or membrane sweeps) can also stir up prostaglandins. This is why a sweep is often offered as a more “natural” induction method during your final prenatal appointments. Once you’ve taken these medications (orally, vaginally, or via IV), more prostaglandins or oxytocin are present in your body and they can then act on their receptors on the uterus muscle.
More reading: What is a Membrane Sweep and Should You Try One?
What are the different types of labor contractions?
Ok, let’s get into the different types of contractions. There are 4 main types of contractions: Braxton Hick’s contractions, prodromal labor contractions, false labor contractions, and true labor contractions. Once you are experiencing true labor contractions, you may also hear those classified based on where you are in the stages of labor. For example, early labor contractions, active labor contractions, transition contractions, and pushing contractions.
What are Braxton Hick’s contractions?
Interestingly, during pregnancy your uterus can actually start contracting as early as 12 weeks. The earliest I ever felt something was at 15 weeks pregnant with my 2nd baby. I still remember it so clearly! I was on a run, so perhaps a little bit dehydrated, and I had a massive contraction. It absolutely stopped me in my tracks. It wasn’t because it was painful, but because I just did not expect to feel something that early!
What I just described to you was a Braxton Hick’s contraction. I’m going to guess you’ve heard something about them at some point! These are “practice” contractions – they are a way your uterus is preparing for its big event. You may or may not feel anything in these early months, but please, don’t worry about that if you don’t. Your body IS practicing, and I’m going to bet that at some point in your third trimester, you may start to notice some BH contractions happening. I also think that once you know what one feels like, you then start to realize you are having them and you just hadn’t realized it up to that point.
What do Braxton Hick’s feel like?
Of course, Braxton Hick’s may feel a little different to everyone. I do think many feel them more from the top of the uterus down (this is me), or as a hardening across the whole belly, as opposed to a lower uterine cramping feeling. Here are some other general characteristics that usually hold pretty true for most:
- Tightening: You can often feel the tightening from the inside and from the outside with your hands.
- Uncomfortable: I always describe them as noticeable or uncomfortable, but not painful.
- Short: Braxton Hick’s are usually brief, typically about 30 seconds max. Occasionally, you may have a massive one (as I did in my story prior), but that was specific to exercise and dehydration for me and wasn’t a “normal” pattern.
- Unpredictable: Braxton Hick’s usually don’t have a rhythm or frequency you can count on, nor do they get closer and closer together. You may experience a few close together, they go away, and then randomly have more a couple hours later.
- Equal: Braxton Hick’s don’t get stronger. Even when you find them pretty dang uncomfortable, they won’t increase in strength.
- Stoppable: You will be able to stop Braxton Hick’s contractions. This usually happens with rest, hydration, stopping exercise, eating, or changing positions.
What causes Braxton Hick’s contractions?
I already mentioned that Braxton Hick’s are your uterus practicing. But there actually are things that you can do that may make them more likely to happen. Braxton Hick’s can be caused by:
- Intercourse: It’s not uncommon to notice Braxton Hick’s contractions after sexual activity, particularly if you have an orgasm.
- Exercise: Many notice more Braxton Hick’s during or after a workout or extra physical activity.
- Dehydration: I know that everyone tells you to drink extra water when pregnant, but it really is so important. Dehydration can cause Braxton Hick’s, and of course, adding in exercise too can really increase your fluid needs.
- Physical Activity: Here, I actually mean activity more related to job or life. Are you on your feet all day for work? Mowing the lawn? Moving into a new home? You may notice more BH during these times.
- Bladder: Raise your hand if you always have to pee right now? I know – you do! Particularly in the third trimester, a full bladder can put pressure on that full uterus and cause some Braxton Hick’s.
I mentioned above that Braxton Hick’s don’t have a predictable rhythm, but I am going to contradict myself really quickly here and say that they can predictably show up during certain consistent patterns in your day. Let me explain.
I had non stop Braxton Hick’s contractions every single time I worked. 13 hour shifts at 37-weeks pregnant are no joke – so I knew to expect lots of Braxton Hick’s, especially by the end of the shift. So, technically, my Braxton Hick’s were pretty darn predictable, in that I knew when they would show up and they consistently did. But, I also knew they would go away as soon as I stopped what was causing them.
How can you get Braxton Hick’s contractions to stop?
So, that is the perfect segue way to the next question: how do you get them to stop? We just went through common causes for Braxton Hick’s. So naturally, you can probably get them to stop by addressing those causes. If you’re noticing a lot of Braxton Hick’s and feeling a little unsure about what’s going on (or just find them super annoying like I do), empty your bladder. Sit down and rest. Drink some water. Consider a position change. Take a shower or a bath. Finish your exercise and rehydrate.
One of the biggest signs of Braxton Hick’s contractions vs true labor contractions is your ability to control them a little bit. If you can’t get them to stop, it may be time to pay a bit more attention to them and see if you’re actually in more of a labor pattern!
What is Prodromal Labor?
Alright, let’s move onto prodromal labor, the next type of contraction. I actually hate teaching about prodromal labor. Why? Because it can be so miserable, and I kind of hate telling you that this could happen to you! But here we are, and it’s a very real thing, so let’s talk about it.
Prodromal labor is interesting in that it is usually more painful than Braxton Hick’s, but still not the “real” thing. You will very likely feel your belly tightening and possibly feel lower uterine pain or back pain. The rhythm of the contractions is usually regular. There is a very good chance you will think these are real (at least when they start)!
In theory, like Braxton Hick’s, prodromal labor is still your body practicing for the real situation. But unlike Braxton Hick’s, you can’t easily make prodromal labor stop, it is painful, and the rhythm can be really regular.
Another important thing to note about this type of contraction is that it does not change your cervix. At some point, prodromal labor often will switch over to true labor (but it can take days). But until that happens, the cervix is not really changing.
How do you get prodromal labor to stop?
To be honest, prodromal labor feels like one of the most frustrating things – and it is often the reason many come into OB triage and then get sent home. We aren’t totally sure what causes prodromal labor, so there aren’t great tips to get it to stop. If you think you are experiencing prodromal labor, you may want to consider an hour or two of gentle activity (like walking) to see if it turns into the real thing. Sometimes, prodromal labor is caused by a baby who is a little crooked in the birth canal (we call that asynclitic), so movement like The Miles Circuit might help get them repositioned better so they can apply more equal pressure to your cervix.
If you’re experiencing prodromal labor, I would mostly encourage you to try and get some rest. Unfortunately, some can have prodromal labor for days, and any rest you can get in the middle of it all will be so helpful when true labor begins.
OB Triage: What Happens and Will You Get Sent Home?
What are false labor contractions?
I just mentioned prodromal labor being one of the common reasons people get sent home from OB triage. Want to know another one? False labor. As you were reading the prior section, you may have been thinking that prodromal labor sounded pretty darn similar to something you already know about called false labor (a lot of people have heard of this type of contraction). But the two are actually different! False labor can begin similarly to prodromal, in that your contractions are consistent, painful, and that you can’t get them to stop on your own, but, there are 2 big differences between the two. This includes:
- False labor stops – on it’s own. It could be an hour or it could be six hours, but all of the sudden, it just stops or fizzles out! Anecdotally, I feel like many experience this in the evenings, lay down to try and get some rest, and at some point fall asleep and wake the next morning to realize it all stopped! Alternatively, prodromal often persists for hours and hours (or even days) before turning into something more.
- False labor can actually change your cervix (remember, prodromal labor doesn’t). Even though it may fizzle out, these contractions can ripen your cervix a bit, which IS helpful for the real event.
I think one of the toughest parts of false labor is if it occurs when you are having a 2nd, 3rd, 4th baby. Typically, we are told to wait at least an hour or more before heading to the hospital with regular contractions. But second babies can come a lot quicker than a first baby! And if I’m being honest, if it was not my first baby, there is likely no way I would wait hours to head to the hospital if I was having strong, close together contractions, just in case it was false labor. This IS what OB triage is for, and if you go in and it’s false labor and you get sent home, there is no shame in that.
What are true labor contractions?
Ok, so it feels like we’ve spent the last 10 minutes talking about everything real labor isn’t. Are you still asking, “but how do I know when my contractions are real?” I get it – that whole “when you know, you know” just doesn’t really feel that comforting.
True labor contractions are the ones that are moving you directly to the main event – baby’s birthday! These are the ones that coincide with cervical change, which means they are moving you towards 10 cm (complete) dilation. Typically, these are going to start sometime after you are 37 weeks pregnant. However, if they begin before you are full term, they would more likely be classified as preterm labor contractions. Depending on how far along you were, your care team may try to stop preterm contractions or they may be okay with the body going for it!
Here are a couple of things that are important to know about real labor:
- True labor doesn’t stop. Contractions may start mild, or really far apart or irregular, but you will start to notice some sort of consistent rhythm through the day (or hours).
- You can’t do anything to get true contractions to stop. Position changes might help you deal with the pain, but they will keep on going through all of it.
- They usually get stronger, longer, and closer together. This isn’t always true (particularly the part about closer together), but it is commonly true.
What do real labor contractions feel like?
I’m going to share some VERY loose classifications of how “true” labor contractions feel. Of course, you have to remember that each of you is SO different in the ways you interpret pain and discomfort, so this may not all hold true for you.
- You often feel true labor contractions in your lower uterine area (like right over your pubis) and/or in your lower back (remember, Braxton Hick’s are commonly a hardening more across the top or around the middle).
- While the details can be nuanced in the pain associated with them, the contractions feel like waves. You can usually feel them coming, they peak, and then they subside.
Recently, I went to my Instagram and polled the community to ask them, in 8 words or less, to describe labor contractions. There were hundreds of comments – some of them made me die laughing, while others made me say “me too.” There are definitely some commonalities in what we experience, but it seems like it’s hard for us to really put it into words too!



How do you time contractions?
You’ve probably picked up on the fact that the rhythm and frequency of contractions is one of the things that can help you decide whether or not your labor is real and when to go to the hospital. Let’s briefly talk about how to time contractions. In preparation of this step in the process, you can print off a paper tracker, download an app, or simply use pen and paper. This is often a great job for the partner – I always handed off the tracker to my husband once early labor was over and I needed to be able to focus a bit more.

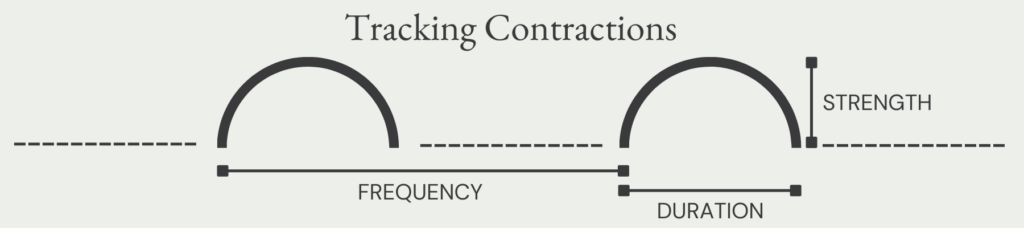
There are three things that commonly get tracked (or charted at the hospital) related to contractions. How far apart are they, how long are they, and how strong are they? To time how far apart contractions are, called frequency, you will want to be tracking from the beginning of one contraction to the beginning of the next. To track how long they are, also called their duration, you want to pay attention to when the contraction begins and when it ends. The strength of the contraction is going to be subjective, and can usually be classified as mild, moderate, or severe or intense. Once you are at the hospital, your RN can also chart the strength of your contractions based on your behavior and/or by feeling your abdomen during one of them.
When to start tracking will be a little bit dependent on you! I like tracking right away, as it helps me pay attention and gives me a little bit of something to anchor myself around. Some like waiting to track until their contractions are a little more consistent, as they find that it is distracting or it makes them focus on their contractions too much. It really is up to you, so my biggest piece of advice is just know how you are going to track, so when you are ready to start, you have what you need.
When should you go to the hospital?
Once you’ve determined your contractions are real, it’s time to consider when you might want to head to the hospital or your birth center.
You may already know the “rule” for when to head in – have you heard of “4-1-1?” Most providers will tell you NOT to head into your birthplace until you are having contractions every 4 minutes, that are 1 minute long, and they’ve been happening for at least 1 hour (sometimes it’s 5-1-1). However, I encourage you to talk to YOUR provider about what they think is best for you. There are a variety of reasons they may change these parameters for you a little bit. This includes things like:
- What birth is this for you? Repeat births often move quicker.
- How far do you live from the hospital? They may want you to head in a bit earlier.
- What are your hopes for pain control? Mamas who desire unmedicated birth may want to hold out a bit longer.
- Is your water broken and/or how long has it been broken? They’ll likely have something to say about that.
- What is your GBS status? If you are positive, remember that means you need some antibiotics before baby is born!
As a nod to your very real intuition too, I want to give you the gentle reminder that if you feel like something doesn’t feel right, please don’t ignore that either (regardless of rules you were given for when to come in)!
Aside from the 4-1-1 or the 5-1-1 rule, I also think it’s really important that you pay attention to what you feel and how it’s changing. If your contractions are still 5 minutes apart but there’s a ton of pressure? That might mean something. Are things way more intense hour to hour even when the frequency is the same? That might mean something! Are you having other signs of labor progress like bloody show or puking? Pay attention! Do you know the emotional signposts? Those will change too and that matters! (Read about The Emotional Signposts of Labor here).
The takeaway on the different types of contractions
It can be so exciting when you first start to feel contractions! I remember that moment from every single one of my births. Equally so, it can be confusing – I remember that too! I hope this blog helps you understand the differences between some of these contractions and will help you make decisions when your own body starts to labor.
If this is the kind of detailed information you want to help you navigate your birth with way more confidence, check out my birth course, Your Body, Your Birth too. Once you join, you’ll have instant access to 13 modules that walk through your pregnancy, birth, and postpartum, giving you access to the information you need to have a much better birth experience!

Did you experience any of these types of contractions? Was it confusing? Did you know when it was real? I’d love to hear about it, so let me know in the comments! xx – Lo
More resources (and freebies!) for you to take a peek at:
- Comprehensive Birth Plan and Birth Priorities templates
- A complete Third Trimester Checklist
- The RN + mama of 4 Ultimate Packing List
- The Labor Mama online birth, baby and breastfeeding classes for every family